Corrective Exercise
Corrective
Strategies for Lumbo-Pelvic-Hip Complex Impairments (LPHC).
The client has problem with lower back pain. She has pelvic tilt and one leg shorter, which means that side is stronger, because it works harder to manage every movement. LPHC is an area of the body which is very important. It has a huge impact on the structures of both upper and lower body. This part of our body contains twenty-nine to thirty-five different muscles that are attached to the lumbar spine or pelvis (Clark et al.,2014). The most important muscles which are associated with the LPHC are: gastrocnemius/soleus, adductor complex, hamstring complex, hip flexor, abdominal complex, erector spinae, intrinsic core stabilizers, latissimus dorsi, tensor fascia latae/ IT band and gluteus medius and maximus. LPHC dysfunction can lead to dysfunctions in the other parts of the body (Powers, 2003). Her upper body has some dysfunction as well which can lead to shoulder and upper – extremity injuries, cervical- thoracic spine and rib cage. Overactivity or tightness of the latissimus dorsi can have unwanted impact on the shoulder. The injury associated with LPHC impairment are lower back pain which the client has already got, sacroiliac joint dysfunction, hamstring complex and groin strains. Injuries which can be on under LPHC are as follows: patellar tendonsitis – ‘jumper’s knee’, IT-band tendonitis- ‘runner’s knee’, medial, lateral, and anterior knee pain, chondromalacia patellae, plantar fasciitis, Achilles’ tendonitis and posterior tibialis tendonitis ‘shin splints’ (Clark et al., 2014). Stress inflicted on the low back can increase hip and spinal flexion. It can also lead to increased stress in the hamstring complex and adductor magnus which can try counterbalance impair gluteus maximus and erector spinae complex to stabilize the LPHC. This leads to hamstring complex and groin strains (Sahrmann, 2002). Overactive can be primary hip flexor as a rectus femoris, which can have impact on ability to lengthen during functional movements and in consequence quadriceps strain and knee pain (Neumann, 2002).
To
improve spine stability, the client should do specific exercises that are used
in rehabilitation and prevention programs. There is a lot of evidence that
exercises are very good for low back pain, however, there are still discussions
about which muscle groups or muscles which are situated closer (local) or
further (global) to also direct exercise
aims during spine stability training (Richardson, 1995).
The
spine stability training is divided into two different approaches, as an
exercise for local muscles contrary to global musculature (Richardson, 1995)
and type of training as improving strength and power (abdominal bracing)
contrary to improving neuromuscular control (abdominal drawing-in maneuver).
The
most popular training uses exercises which concentrated on the global
stabilizers. One study suggests that for spine stability the most important
muscles are global (Grieve, 1982), however, this study presumes that
intervertebral stability is accomplished. There was a discussion about which
muscles local or global, are more helpful in spine stability. The conclusion is
that both of muscles are engaged in spine stability, both of them bracing and
drawing-in, which has an impact on intervertebral stability and lumbopelvic
stability. The lumbopelvic stability relies on intervertebral stability. To
train the local muscles and improve intervertebral stability basis is to the
drawing-in movement. It can be a start in spine stability training program and it
can progress to abdominal bracing (Richardson, 1995).
The
client has got static posture assessment and she has lower crossed syndrome,
because she has anterior pelvic tilt. The pelvis and lumbar spine are in
position where there is excessive stress on the muscles and connective tissue
related to LPHC during dynamic movement. She did single-leg squats and her
torso has rotated inwards and hip has hiked.
After dynamic Postural Assessment, Gait: Treadmill Walking is known that
she has excessive pelvic rotation. Suggested training program:
Self-Myofascial Release
Here
are exercises which the client should to: inhabit by foam rolling. Both sides:
side toward shift (adductor and TFL/IT-band and opposite side away from shift
piriformis and biceps femoris. In this situation gastrocnemius and soleus are
big factor as well. The client did squat, and while she was down here ankle
joints lacks sagittal plane dorsiflexion, this pushes the body to shift away
from the limited side and shift to the other side. Suggested: hold on for
thirty seconds.
Figure 1: Same side
TFL/IT-Band
 (Google.com, 2019)
(Google.com, 2019)
Figure 2: Opposite side Piriformis

(Google.com, 2019)

Figure 3: Same Side Adductors


(Google.com, 2019)
Figure 4: Opposite Side Biceps Femoris

(Google.com, 2019)
Figure 5: Opposite Side Biceps Femoris


(Google.com, 2019)
Static
Stretches
Next
very important part is lengthening by static and neuromuscular stretches. The
same side adductors and opposite gastrocnemius/soleus, TFL/IT-band, biceps
femoris, and piriformis. Suggested: hold on for thirty seconds or can be for
seven to ten seconds isometric contraction, and hold on for thirty seconds
again.
Figure 6:
Same Side Adductors

(Google.com, 2019)
Figure 7: Opposite Side Gastrocnemius/Soleus
 (Google.com, 2019)
(Google.com, 2019)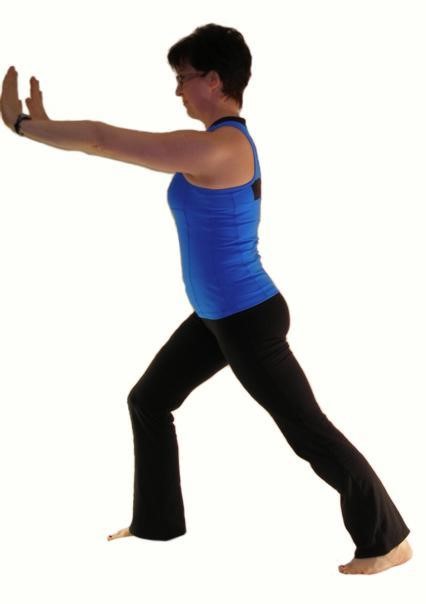
Figure 8: Same Side TFL

 (Google.com, 2019)
(Google.com, 2019)
Figures
9:
Opposite Side Piriformis

 (Google.com, 2019)
(Google.com, 2019) (Google.com, 2019)
(Google.com, 2019)
Figure
10:
Opposite Side Biceps Femoris

 (Google.com, 2019)
(Google.com, 2019)
Neuromuscular Stretches: a second person is
needed

 (Google.com, 2019)
(Google.com, 2019)
Figure 12 Piriformis: Same
Side Adductors


 (Google.com, 2019)
(Google.com, 2019)
Figure 13: Opposite Side Biceps Femoris

 (Google.com, 2019)
(Google.com, 2019)
Isolated
Strengthening Exercises they will activate body by isolated strengthening
exercises and positional isometrics. The same side gluteus medius and the
opposite side adductor complex. The client can make 4 repetition of increasing
intensity 25, 50, 75 and 100% or 10-15 repetition with 2 seconds isomeric hold
and 4 seconds eccentric contraction.
Figure 14: Opposite side adductor complex


 (Google.com, 2019)
(Google.com, 2019)
Figure 15: Same side Gluteus Medius


 (Google.com, 2019)
(Google.com, 2019)
Positional Isometric Techniques - second person
needed
Figure 16: Same Side Gluteus Medius


 (Google.com, 2019)
(Google.com, 2019)
Figure 17: Opposite Side Adductor Complex


 (Google.com, 2019)
(Google.com, 2019)
Integrate exercise, dynamic movement. The client can use ball and
make wall squats with dumbbells 10-15 repetition. Hold proper position to
control exercise.
Figure 18: Wall Squat



 (Google.com, 2019)
(Google.com, 2019)
For flat feet’s, she should
walk on her toes, heels and inner side of the feet for a few minutes daily. She
should use orthopaedical shoe insoles to be on the same level as the right part
on her body. The left shorter leg will have support and this can be helpful for
LPHC impairment.
References
·
Google.com. (2019). ball wall squats to
overhead press - Google Search. [online] Available at:
https://www.google.com/search?safe=strict&tbm=isch&source=hp&biw=1242&bih=592&ei=koDhXKK_CYfYaaeVr8gF&q=ball+wall+squats+to+overhead+press&oq=ball+wall+squats+to+overhead+press&gs_l=img.3...4994.23559..23789...0.0..0.207.2154.30j3j1......3....1..gws-wiz-img.....0..0j0i5i30j0i8i30j0i24j0i30.qeqFlFHAVzw#imgrc=MZUqupNSPxa2aM:
[Accessed 19 May 2019].
·
Michael A. Clark, Scott C. Luccet, Brian G.
Sutton (2014). Corrective Exercise Training Knee. 28(5),
pp309-337.
·
Neuman DA (2002). Kinesiology of the Musculoskeletal System: Foundations for Physical
Rehabilitation. St Louis: Mosby.
·
Powers CM, (2003). The influence of altered-
lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical
perspective. J Orthop Sports Phys Ther .
2003;33(11):639-646.
·
Richardson C, Jull G, Hodges P, Hides, (1999). Therapeutic
Exercise for Spinal Segmental Stabilization in Low Back Pain. London: Churchill
Livingstone.
·
Sahramann SA (2002). Diagnosis and Treatment of Movement Impairment Syndromes. St.
Louis: Mosby, Inc;

This is a really informative knowledge, Thanks for posting this informative Information. Pre and post natal training
OdpowiedzUsuń